
Atrial Fibrillation
A clear, reassuring guide to what atrial fibrillation (AF/AFib) means, why it can increase stroke risk, how it may be picked up, and why proper diagnosis matters.
Last reviewed: May 2026
Most of the time, your heart beats in a steady, organised rhythm without you needing to think about it.
But sometimes that rhythm becomes irregular. Atrial fibrillation — often shortened to AF or AFib — is one common reason this can happen, especially as people get older.
AF can cause palpitations, breathlessness, tiredness, or an uncomfortable awareness of the heartbeat. But it can also be silent, with no clear symptoms at all.
Because AF is common, particularly in later life, it is worth understanding properly rather than guessing from symptoms alone.
This page explains what AF is, why it matters, how it may be picked up, and why proper diagnosis matters.
Quick overview
What is atrial fibrillation?
Atrial fibrillation is a heart rhythm condition where the upper chambers of the heart (atria) stop following their usual, organised electrical pattern.
Video showing the electrical signal during a normal regular rhythm.
In AF, that organised pattern breaks down. Instead of one clear signal, there are many rapid, disorganised electrical signals. The atria no longer squeeze in the usual coordinated way. They may quiver, or fibrillate, instead.
The lower chambers (ventricles) still do most of the pumping work. But because the signals reaching them are uneven, the pulse often becomes irregular. In some people, the heartbeat may also become faster than usual.
In a normal rhythm, each heartbeat begins with a clear electrical signal high in the heart, helping the upper and lower chambers work together in an efficient sequence.
This signal spreads smoothly across the atria, helping them squeeze and move blood down into the lower chambers before the main pumping action begins.
Our page on how the heart works explains this normal electrical timing in more detail.
Video showing the disorganised electrical signals during atrial fibrillation.
This is why atrial fibrillation is often noticed as an irregular heartbeat. But AF is not just a feeling. It is a specific rhythm condition that needs proper assessment.
Is atrial fibrillation the same as an irregular heartbeat?
Not exactly.
An irregular heartbeat is a general description. It means the timing of the beats is not following its usual steady pattern. There are different reasons this can happen, and not all of them are atrial fibrillation.
Atrial fibrillation is one specific type of irregular heart rhythm. In AF, the problem begins in the atria, where the electrical activity becomes disorganised.
Regular rhythm and atrial fibrillation: a simplified comparison
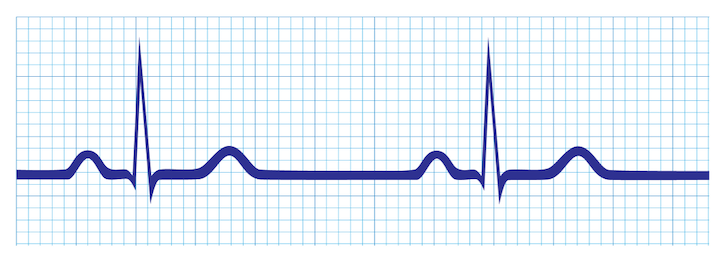
ECG-style illustration of a normal, regular heart rhythm, where the beats follow a steady pattern.
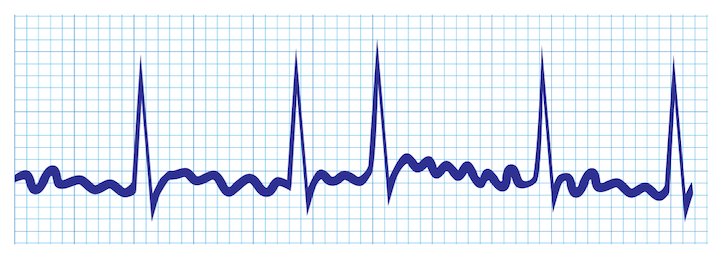
ECG-style illustration showing how atrial fibrillation can produce an irregular rhythm pattern.
These simplified ECG-style illustrations are for general education only. They are not diagnostic ECG examples. Atrial fibrillation can only be confirmed through proper ECG-based assessment and medical interpretation.
A simple way to think about it is this:
Irregular heartbeat describes what may be noticed.
Atrial fibrillation describes one possible cause.
That distinction matters because an irregular pulse is a clue, not a diagnosis. Fluttering, an uneven pulse, or a home-device alert does not prove that AF is present. Equally, having few or no symptoms does not rule AF out.
What can atrial fibrillation feel like?
Atrial fibrillation can feel different from person to person.
Some people notice a clear change in their heartbeat. It may feel as though the heart is fluttering, racing, thumping, or beating unevenly, sometimes in the chest, throat, or neck.
AF can also cause symptoms that do not immediately feel like a rhythm problem, such as unusual tiredness, breathlessness, light-headedness, chest discomfort, or reduced ability to manage normal activity.
These symptoms may happen because the heartbeat is irregular, sometimes faster than usual, and not always as efficient as a steady, organised rhythm.
But AF does not always announce itself clearly. Some people have no obvious palpitations at all. They may only find out when their pulse is checked, a home device raises an alert, or an ECG (electrocardiogram) is performed during a routine appointment.
The strength of symptoms does not always show how important the rhythm change is. New, repeated, or unexplained symptoms should not be dismissed.
Can atrial fibrillation come and go?
Yes. Atrial fibrillation does not always stay present all the time.
For some people, AF happens in episodes. The rhythm may become irregular for minutes, hours, or longer, and then return to normal. Because it comes and goes, it may not be present during a routine appointment or short ECG recording.
This intermittent pattern is one reason AF can be difficult to capture. A person may feel symptoms at home, but by the time they are checked, the rhythm has settled.
For other people, AF becomes more persistent. It may last longer, happen more often, or become the person’s usual rhythm over time.
If AF is suspected but not captured straight away, a healthcare professional may recommend further rhythm monitoring.
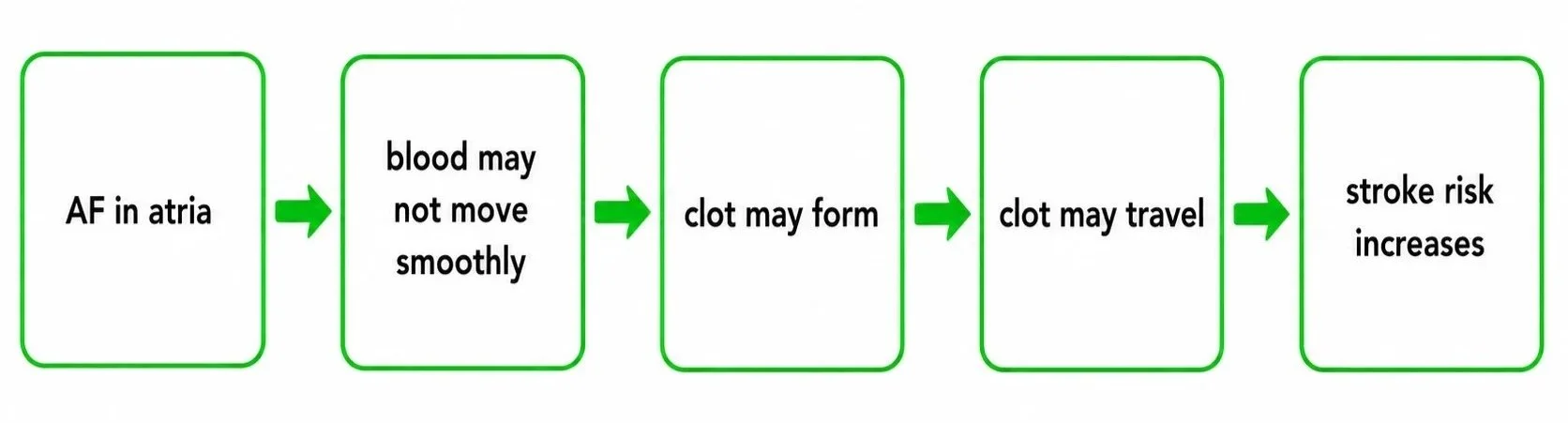
How does atrial fibrillation increase stroke risk?
Atrial fibrillation can affect more than how the heartbeat feels.
For some people, AF causes symptoms that affect confidence, sleep, exercise, and everyday activity. But one of the main reasons AF needs proper attention is its link with stroke risk.
In AF, the atria are not squeezing in their usual organised way. Blood may not move through them as smoothly as it should. When blood flow becomes sluggish, there is a greater chance that a clot could form inside the heart. If a clot travels to the brain, it can block blood flow and cause an ischaemic stroke.
That does not mean everyone with AF has the same level of risk. Stroke risk depends on factors such as age, blood pressure, diabetes, a previous stroke or blood clot, heart failure, and overall health history.
This is why proper assessment matters. It helps healthcare professionals judge the level of risk and decide whether treatment to reduce that risk is needed.
The reassuring part is that AF is often manageable once recognised. Diagnosis does not mean panic. It means the rhythm, stroke risk, and treatment options can be considered properly.
Who is more likely to develop atrial fibrillation?
Atrial fibrillation can happen to adults of different ages, but it becomes more common as people get older.
That does not mean AF is an inevitable part of ageing. It simply means the chance of developing it rises over time, especially when the heart and blood vessels have been exposed to strain for many years.
Several factors can make AF more likely. These include:
increasing age
high blood pressure
heart disease, heart failure, or a previous heart attack
heart valve problems
diabetes
being overweight or living with obesity
an overactive thyroid
sleep apnoea
smoking or higher alcohol intake
some medicines or stimulants
High blood pressure deserves particular attention because it is common, often silent, and closely linked with long-term strain on the heart.
Episodes of AF may sometimes be noticed after alcohol, illness, stress, poor sleep, dehydration, or heavy exertion.
It is also possible to develop AF without an obvious cause. Risk factors can guide awareness, but they cannot diagnose the rhythm.
How is atrial fibrillation picked up?
Atrial fibrillation can be picked up in different ways.
Sometimes the first clue is how a person feels: palpitations, breathlessness, tiredness, dizziness, chest discomfort, or a sudden change in normal activity levels.
Sometimes the first clue is the pulse. A healthcare professional may feel the pulse at the wrist and notice that it is irregular. Some people notice this themselves.
AF may also be suspected during a routine appointment, blood pressure check, or assessment for another health problem. Home devices can raise awareness too, including some blood pressure monitors, smartwatches, and ECG-capable devices.
These clues can be useful, especially when AF comes and goes. But they are prompts for further assessment, not final answers.
A symptom, pulse check, or device alert may raise suspicion.
An ECG-based assessment is usually needed to confirm what the rhythm actually is.
How is atrial fibrillation diagnosed?
Atrial fibrillation is diagnosed by recording the heart’s electrical activity and showing that AF is present.
The usual test is an ECG (electrocardiogram). An ECG records the electrical signals of the heart and displays them as a tracing, allowing a healthcare professional to assess the rhythm directly.
If an irregular pulse is found and AF is suspected, a standard ECG may be performed. This is often called a 12-lead ECG. It is quick and painless, and involves small sticky sensors placed on the skin of the arms, legs, and chest.
The challenge is that AF is not always present at the exact moment the ECG is recorded. If it comes and goes, a short ECG recording may look normal even if the person has been having episodes at other times.
In that situation, longer monitoring may be needed, such as wearing a portable heart monitor for 24 hours, several days, or longer. The aim is to capture the rhythm during an episode, rather than guessing from symptoms alone.
A diagnosis of AF should not be based only on how the heartbeat feels, a pulse check, or a home-device alert. These can point someone in the right direction, but a diagnosis needs ECG-based evidence and medical interpretation.
How atrial fibrillation is treated and managed
Treatment for atrial fibrillation depends on the person, their symptoms, how long AF has been present, and their wider stroke and bleeding risk.
Once AF is confirmed, management usually focuses on three broad questions.
First, does the person need treatment to reduce stroke risk? If the risk is high enough, anticoagulant medicine may be recommended. These medicines reduce the blood’s ability to clot, lowering the chance that a clot will form and travel to the brain.
Second, does the heart rate need controlling? Some people with AF have a heart rate that is too fast, especially during episodes. Medicines may be used to slow the heart rate, reduce strain on the heart, and improve symptoms.
Third, should treatment try to restore or maintain a normal rhythm? For some people, treatment may focus on rhythm control, using medicines or specialist procedures depending on symptoms, AF pattern, heart health, and specialist assessment.
Management may also include looking for factors that can make AF harder to control, such as high blood pressure, thyroid problems, sleep apnoea, alcohol intake, weight, or other heart conditions.
The important message is that AF is often manageable. A diagnosis does not automatically mean dramatic intervention, but the rhythm and stroke risk should be properly assessed.
Can a blood pressure monitor detect atrial fibrillation?
Some home blood pressure monitors can detect an irregular pulse pattern during a reading. Some models also include a more specific feature designed to flag possible atrial fibrillation.
These features can be useful, especially because AF can be silent or can come and go. But they need careful interpretation.

A standard home blood pressure monitor does not record the heart’s electrical activity in the way an ECG does.
It estimates blood pressure by detecting pulse waves in the artery while the cuff inflates and deflates. If those pulse waves arrive unevenly, the device may recognise an irregular pattern.
That means a blood pressure monitor may raise suspicion, but it cannot confirm AF on its own.
It is also important to understand the difference between two types of alert:
a general irregular heartbeat symbol means the pulse seemed uneven during the reading
a possible AF/AFib alert is designed to look for a pattern that may suggest atrial fibrillation
Neither should be ignored if repeated, but neither is the same as a diagnosis. Movement, talking, cuff problems, extra beats, or other rhythm changes may also affect the reading.
In simple terms:
A blood pressure monitor may help notice a possible rhythm problem.
It cannot diagnose atrial fibrillation.
Key takeaways: atrial fibrillation explained
Atrial fibrillation is a specific type of irregular heart rhythm that begins in the upper chambers of the heart.
AF can cause palpitations, breathlessness, tiredness, dizziness, or an uncomfortable awareness of the heartbeat, but it can also cause no obvious symptoms at all.
AF may come and go, so it is not always captured during a short appointment or single ECG recording.
AF matters because it can increase the risk of blood clots forming inside the heart, which can increase stroke risk in some people.
A pulse check, home blood pressure monitor, smartwatch, or ECG-capable device may raise suspicion, but proper diagnosis usually requires ECG-based evidence and medical interpretation.
AF is often manageable once it is recognised, assessed, and treated appropriately.
When to seek medical help
This content is for general education only and does not diagnose atrial fibrillation or provide medical advice.
If you notice a new, repeated, or unexplained irregular heartbeat, or if you have palpitations, breathlessness, unusual tiredness, dizziness, or a sudden drop in normal activity levels, speak with your doctor or another qualified healthcare professional.
If a home blood pressure monitor, smartwatch, or other device repeatedly shows an irregular heartbeat or possible AF/AFib alert, it is sensible to arrange a medical assessment. A device alert does not confirm AF, but it may be an important clue.
If an irregular heartbeat comes with chest pain, fainting, severe breathlessness, symptoms of a stroke, or if you feel suddenly very unwell, seek urgent medical help.
This page can help you understand what AF may mean, but it cannot tell you whether AF is present in an individual case. That needs proper medical assessment.
If you would like to understand the broader topic first, our Irregular Heartbeat page explains what an irregular heartbeat can mean and how it differs from atrial fibrillation.
If you would like to understand home monitoring in more detail, our Blood Pressure Monitors Guide explains how home blood pressure monitors work, what rhythm-related features they may include, and what to consider when choosing a device.
Important Information:
This page is provided for general educational purposes only and does not constitute medical advice. Medical knowledge and guidance evolve over time, and information may change. Always seek advice from a qualified healthcare professional regarding personal health concerns or medical decisions.
For more details, please see our full Disclaimer.